
 In the ’70s and early ’80s, in his outstanding TV criticism in the Observer, Clive James had an unfailing ear for the peculiarities of American pronunciation. Facing David Frost’s sing-song questions, Henry Kissinger fell bag on swapping his DTs and CGs. Meeting Frost’s aria-ettes on Vietnam with the sound of gravel being forced through a hand mincer, Big K conceded that ‘manipulading the domesdig affairs of another gountry is always gombligaded’. On Chile, where the Americans had been up to their usual tricks, Kissinger explained it was down to a certain ‘peculiaridy of the consdidution’. On another occasion a year later, asked what he and Reagan had discussed pre-election, Kissinger revealed the devastating charm of his verbal dricks. ‘I jusd wished him good lug’. No wonder Hopalong won.
In the ’70s and early ’80s, in his outstanding TV criticism in the Observer, Clive James had an unfailing ear for the peculiarities of American pronunciation. Facing David Frost’s sing-song questions, Henry Kissinger fell bag on swapping his DTs and CGs. Meeting Frost’s aria-ettes on Vietnam with the sound of gravel being forced through a hand mincer, Big K conceded that ‘manipulading the domesdig affairs of another gountry is always gombligaded’. On Chile, where the Americans had been up to their usual tricks, Kissinger explained it was down to a certain ‘peculiaridy of the consdidution’. On another occasion a year later, asked what he and Reagan had discussed pre-election, Kissinger revealed the devastating charm of his verbal dricks. ‘I jusd wished him good lug’. No wonder Hopalong won.
Coercive Healthism
The Blind Archer
 Hell may have no fury greater than a woman scorned, but surely Heaven can have no joy greater than a woman reformed. In a remarkable development, scientists in North America have popped not a bun but a biodegradable scaffold layered with a patient’s vulval and other cells in the oven, and after the required time at the requisite temperature been rewarded with a fully formed vagina. Four women born without a vagina have had ready-vaginas made this way implanted, and have subsequently reported normal or even atomic levels of ‘desire, arousal, satisfaction and orgasm’. This extraordinary advance may in the short term pave the way for a gruesome commerce in designer vaginas – each scaffold is individually crafted - but in time it can only end one way: the day will dawn when we pop not buns but homunculi in the oven, to be rewarded nine months later with little incubi, all of whom will go on to report normal or even atomic levels of desire, arousal, satisfaction and orgasm. Truly, science knows no bounds.
Hell may have no fury greater than a woman scorned, but surely Heaven can have no joy greater than a woman reformed. In a remarkable development, scientists in North America have popped not a bun but a biodegradable scaffold layered with a patient’s vulval and other cells in the oven, and after the required time at the requisite temperature been rewarded with a fully formed vagina. Four women born without a vagina have had ready-vaginas made this way implanted, and have subsequently reported normal or even atomic levels of ‘desire, arousal, satisfaction and orgasm’. This extraordinary advance may in the short term pave the way for a gruesome commerce in designer vaginas – each scaffold is individually crafted - but in time it can only end one way: the day will dawn when we pop not buns but homunculi in the oven, to be rewarded nine months later with little incubi, all of whom will go on to report normal or even atomic levels of desire, arousal, satisfaction and orgasm. Truly, science knows no bounds.
The Invisible Gorilla
 Statins continue to generate more heat than light. On the Today programme this morning, the pro-statin academic Sir Rory Collins only just managed to get off at Edge Hill rather than go on to accuse BMJ editor Dr Fee of mass murder for publishing research suggesting statins for people at low risk of heart disease may do more harm than good. The bun-fight is interesting because in the heat we do in fact find some light shone on a blind sector in gold-standard drug research: we tend to see what we are looking for, which means we tend not to see what we are not looking for, an effect known as the Invisible Gorilla effect. A well known example is the sexual side effects of the SSRI anti-depressants. Because initial clinical trials were conducted on healthy volunteers (often stoodents) with male libidos the size of the Eiffel Tower, no one thought to look for sexual side effects. But once SSRIs got out into the wild, it became apparent that what had once been two foot long and hard as steel was now measured in inches and made of jelly. Once unwanted SSRI sexual side-effects are looked for, it turns out SSRIs are to your sex life what a water hose is to your bonfire.
Statins continue to generate more heat than light. On the Today programme this morning, the pro-statin academic Sir Rory Collins only just managed to get off at Edge Hill rather than go on to accuse BMJ editor Dr Fee of mass murder for publishing research suggesting statins for people at low risk of heart disease may do more harm than good. The bun-fight is interesting because in the heat we do in fact find some light shone on a blind sector in gold-standard drug research: we tend to see what we are looking for, which means we tend not to see what we are not looking for, an effect known as the Invisible Gorilla effect. A well known example is the sexual side effects of the SSRI anti-depressants. Because initial clinical trials were conducted on healthy volunteers (often stoodents) with male libidos the size of the Eiffel Tower, no one thought to look for sexual side effects. But once SSRIs got out into the wild, it became apparent that what had once been two foot long and hard as steel was now measured in inches and made of jelly. Once unwanted SSRI sexual side-effects are looked for, it turns out SSRIs are to your sex life what a water hose is to your bonfire.
Nice Try, But No Cigar
 The front door, or rather back door, tactics of the shadowy Health and Social Care Information Centre have achieved a sort of slow-burn blowback over the last few weeks. Kicked off with a junk mail leaflet that aimed to be funky but turned out flakey – eye catching shape, double helix on the front, but the helix unravelling on the inside, and written by a Kafkaesque we who never said who we were, in opaque prose that bizarrely got a Crystal Mark for Clarity from the Plain English Campaign – the idea was to have patients default into allowing the NHS to hoover personally identifiable GP medical records into a vast data silo the size of Russia, generally for the purposes of improving care. But that was only part of it. Buried in the flyer, we also had plans to flog off your data, including sometimes personally identifiable so called red data, but only after the strictest approvals, you understand. Or at least we did. Whether the rest of us did was another matter.
The front door, or rather back door, tactics of the shadowy Health and Social Care Information Centre have achieved a sort of slow-burn blowback over the last few weeks. Kicked off with a junk mail leaflet that aimed to be funky but turned out flakey – eye catching shape, double helix on the front, but the helix unravelling on the inside, and written by a Kafkaesque we who never said who we were, in opaque prose that bizarrely got a Crystal Mark for Clarity from the Plain English Campaign – the idea was to have patients default into allowing the NHS to hoover personally identifiable GP medical records into a vast data silo the size of Russia, generally for the purposes of improving care. But that was only part of it. Buried in the flyer, we also had plans to flog off your data, including sometimes personally identifiable so called red data, but only after the strictest approvals, you understand. Or at least we did. Whether the rest of us did was another matter.
Left Shit
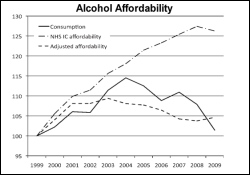
 The title for this post arises because Dr No has idly been playing Shorter Titles, the I’m Sorry I haven’t A Clue game in which panellists are invited to submit film (or song) titles where a single letter omission changes the meaning – Oldfinger, The King’s Peech, Rear Widow, The Godfarter, The Tird Man, that sort of thing – but as Jack Dee would say, they don’t work in print - the original title here being Left Shift, the hypothetical statistical fancy much beloved of the medical Islingtonistas who favour alcohol minimum unit pricing. Left shift is the notion that in populations the body wags the tail: the mean determines the extremes. Applied to alcohol minimum pricing, left shift has it that if average consumption falls because of raised minimum unit prices, then so too will heavy consumption fall. Populations, according to this hypothesis, behave like a blancmange made with excess gelatine: a nudge in the middle, and the whole pud moves across.
The title for this post arises because Dr No has idly been playing Shorter Titles, the I’m Sorry I haven’t A Clue game in which panellists are invited to submit film (or song) titles where a single letter omission changes the meaning – Oldfinger, The King’s Peech, Rear Widow, The Godfarter, The Tird Man, that sort of thing – but as Jack Dee would say, they don’t work in print - the original title here being Left Shift, the hypothetical statistical fancy much beloved of the medical Islingtonistas who favour alcohol minimum unit pricing. Left shift is the notion that in populations the body wags the tail: the mean determines the extremes. Applied to alcohol minimum pricing, left shift has it that if average consumption falls because of raised minimum unit prices, then so too will heavy consumption fall. Populations, according to this hypothesis, behave like a blancmange made with excess gelatine: a nudge in the middle, and the whole pud moves across.
Supping With a Short Spoon
 Just as there is gold for drug companies in them thar pills, so there is gold for GPs in them thar patients. Historically, GPs were paid chiefly on a patient head-count basis, topped up with item of service fees for ‘extras’ such as vaccinations and contraception. The simplest way for GPs to boost income under this system was to increase list size, sometimes to absurd levels where the GP could not hope to provide adequate care for all the patients on the list. Some even gamed the system, by sneaking ghost patients on their lists. Governments disliked crude head-count based pay, not least because it offered no scope to influence GP activity. Item of service payments were an attempt to change that, but the capitation fee was still paid whatever the doctor did, or didn’t, do. The below par golfing GP trousered the fee in equal measure to his more conscientious colleague on the other side of town.
Just as there is gold for drug companies in them thar pills, so there is gold for GPs in them thar patients. Historically, GPs were paid chiefly on a patient head-count basis, topped up with item of service fees for ‘extras’ such as vaccinations and contraception. The simplest way for GPs to boost income under this system was to increase list size, sometimes to absurd levels where the GP could not hope to provide adequate care for all the patients on the list. Some even gamed the system, by sneaking ghost patients on their lists. Governments disliked crude head-count based pay, not least because it offered no scope to influence GP activity. Item of service payments were an attempt to change that, but the capitation fee was still paid whatever the doctor did, or didn’t, do. The below par golfing GP trousered the fee in equal measure to his more conscientious colleague on the other side of town.
Most Drugs Don’t Work
 Just over three years ago, when few had heard of him, Dr No wrote a post called The Collapse of the Probability Function. At its heart lies the troublesome paradox that, while we might know how a group of patients might fare, we have no way of knowing how individual patients will fare. We might know that of a hundred patients, five will die in the next ten years from a heart attack. What we don’t know is who of the hundred will be the five; and the flip side of that is, when as doctors we choose to intervene, as increasingly we do, there are ninety five souls now tangled in our medical web, with all that that entails, be it tests, treatments and general apprehension, who were never going to have a heart attack anyway, let alone die from one in the next ten years. That’s a whole lot of medical intervention without any benefit whatsoever – but what the heck – overall, we might save a handful of lives - or so the hopeful reasoning goes.
Just over three years ago, when few had heard of him, Dr No wrote a post called The Collapse of the Probability Function. At its heart lies the troublesome paradox that, while we might know how a group of patients might fare, we have no way of knowing how individual patients will fare. We might know that of a hundred patients, five will die in the next ten years from a heart attack. What we don’t know is who of the hundred will be the five; and the flip side of that is, when as doctors we choose to intervene, as increasingly we do, there are ninety five souls now tangled in our medical web, with all that that entails, be it tests, treatments and general apprehension, who were never going to have a heart attack anyway, let alone die from one in the next ten years. That’s a whole lot of medical intervention without any benefit whatsoever – but what the heck – overall, we might save a handful of lives - or so the hopeful reasoning goes.
Most Drugs Don’t Work
Just over three years ago, when few had heard of him, Dr No wrote a post called The Collapse of the Probability Function. At its heart lies the troublesome paradox that, while we might know how a group of patients might fare, we have no way of knowing how individual patients will fare. We might know that of a hundred patients, five will die in the next ten years from a heart attack. What we don’t know is who of the hundred will be the five; and the flip side of that is, when as doctors we choose to intervene, as increasingly we do, there are ninety five souls now tangled in our medical web, with all that that entails, be it tests, treatments and general apprehension, who were never going to have a heart attack anyway, let alone die from one in the next ten years. That’s a whole lot of medical intervention without any benefit whatsoever – but what the heck – overall, we might save a handful of lives - or so the hopeful reasoning goes.
Gluganomics
 Today’s announcement by Scotland’s Minister for Emesis, Nicola Stugeron, that the Scottish government intends to set a 50p minimum unit price for alcohol reminds Dr No that a similar bell is set to toll South of the Border. Forty-eight hours after Porgie’s boomerang budget, the one that keeps on coming back to tap the Tories where it hurts, Theresa May was pushed on to the floor of the Commons, in a reckless bigger-the-pushed’un-the-better-the-cushion move, to zap hostile media coverage of the budget, by announcing the Westminster government’s own Alcohol Strategy. Needless to say, that strategy also contains proposals for minimum unit pricing, and, needless to say, both governments are equally deluded in their expectations that this daft policy will do any good. In fact, Dr No predicts it may even do harm.
Today’s announcement by Scotland’s Minister for Emesis, Nicola Stugeron, that the Scottish government intends to set a 50p minimum unit price for alcohol reminds Dr No that a similar bell is set to toll South of the Border. Forty-eight hours after Porgie’s boomerang budget, the one that keeps on coming back to tap the Tories where it hurts, Theresa May was pushed on to the floor of the Commons, in a reckless bigger-the-pushed’un-the-better-the-cushion move, to zap hostile media coverage of the budget, by announcing the Westminster government’s own Alcohol Strategy. Needless to say, that strategy also contains proposals for minimum unit pricing, and, needless to say, both governments are equally deluded in their expectations that this daft policy will do any good. In fact, Dr No predicts it may even do harm.
Calling Time on Minimum Pricing
 Once again, the brown trout that wont flush away has bobbed up for air. Yesterday, David Cameron put alcohol minimum pricing back on the agenda. Across the land, responsible doctors cried Cheers! The Chair of the Royal College of General Practitioners, Dr Clare Gerada, who counts addiction – in others, one hastens to add – among her special interests, spoke for many when she tweeted the price, availability and advertising is all mantra. This mantra is underpinned by left shift, which sounds cool, being the sort of thing cool astronomers like Brian ‘Wow, Magnificent’ Cox might say, but it suffers from a defect WM would never allow: it is chasing the wrong hair, or rather tail, of the dog. In practice, minimum pricing will be spectacularly ineffective at reducing high alcohol use, and even worse, it will almost certainly result in blowback, by which Dr No refers not to the visit to the loo on the morning after the night before, but unintended harm arising from well-intentioned practice.
Once again, the brown trout that wont flush away has bobbed up for air. Yesterday, David Cameron put alcohol minimum pricing back on the agenda. Across the land, responsible doctors cried Cheers! The Chair of the Royal College of General Practitioners, Dr Clare Gerada, who counts addiction – in others, one hastens to add – among her special interests, spoke for many when she tweeted the price, availability and advertising is all mantra. This mantra is underpinned by left shift, which sounds cool, being the sort of thing cool astronomers like Brian ‘Wow, Magnificent’ Cox might say, but it suffers from a defect WM would never allow: it is chasing the wrong hair, or rather tail, of the dog. In practice, minimum pricing will be spectacularly ineffective at reducing high alcohol use, and even worse, it will almost certainly result in blowback, by which Dr No refers not to the visit to the loo on the morning after the night before, but unintended harm arising from well-intentioned practice.